Are Geophysics Dramatically Changing COVID19 Outcomes in Some Locations? We May Find Out the Hard Way March 2021.

2020 has shown us our normal tools for understanding and solving respiratory virus pandemics are just not working for COVID19 and some aspects of the spread, mechanisms and fatality make no logical sense. Is it possible that geophysics are coupled to fatality rates and long term outcomes? The researchers that predicted this pandemic think so. The announcement of a spontaneous peak of deaths peaking in mid March and following the death pattern of 2020, will be the ultimate validation.
There seem to be a lot of counter-intuitive aspects of COVID19 that have researchers scratching their heads. Remdesivir, the anti-viral which received FDA fast track approval as the first drug for treating COVID19, was found to be useless for improving COVID19 fatality and the World Health Organization almost immediately issued a recommendation against its use. Intubation, the common intervention for respiratory failure, has shockingly low survival rates — 70% or more of patients that have received intubation die on average. This is highly counter-intuitive with current understanding, leading many doctors and researchers to speculate that the respiratory failure is actually a bio-energetic issue, oxygen is not transferring to the blood, almost like altitude sickness or high altitude pulmonary oedema. Its become clear that COVID19 is not really a pneumonia at all, but some type of complex blood disease causing systematic effects in most organs — somehow without ever leaving behind tell-tale viral RNA in the locations of damage like all other viruses.
SARS-CoV-2 viral load has been shockingly low, with PCR tests requiring 40+ PCR cycles to find viral presence, well beyond the unofficial 35 PCR cycle standard Dr. Anthony Fauci mentioned in a recent interview for “replication competent” viruses and not “just dead nucelotides, period”. The epidemiology makes no sense, with the virus spontaneously exploding into widespread disease across the world in the same months, yet seemingly not killing people regardless of distancing measures entire land masses like India, Africa, Australia and most of Asia. SARS-CoV-2 antibodies found in hundreds of patient blood samples in Italy, months before it was identified in Wuhan. Spontaneous and unique lung damage and loss of smell in even mildly symptomatic patients points to a non-linear and systematic progression of disease. Risk factors for COVID19 are metabolic disorders like diabetes and obesity, not immune strength, lung function or other common sense co-morbidities — indicating a reliance on the bodies bioenergetic system.
CAUTION: This is speculation and is not advice that contradicts any public health measures such as PPE, social distancing or other initiatives. This is forward looking research and should not be used in place of government mandates and public health stakeholder advice!
Going back to basics with the benefit of hindsight — who predicted a 2020 respiratory disease pandemic? Only one group of people predicted this pandemic: those studying the influence of planetary physics on disease outbreaks. In January 2019, as the coronavirus started to take hold in Wuhan, a world class astrobiologist saw the writing on the wall and published an interview, “Coronavirus could turn to global pandemic as freak solar minimum means outbreak ‘imminent’”
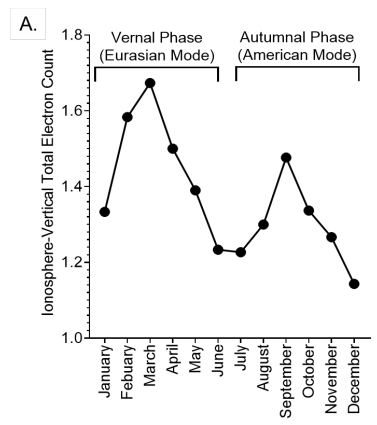
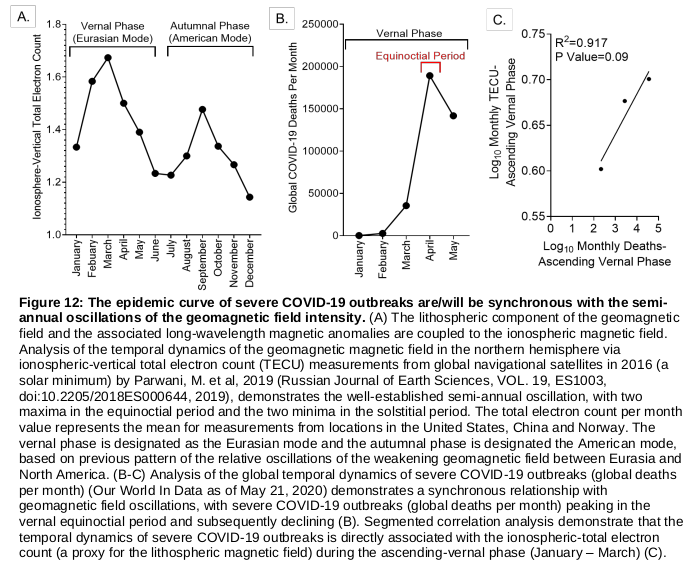
Multiple researchers predicted higher incidences of disease as the sun went into a solar minimum, particularly on the equinoxes, when the ionosphere is weakest and earth is being hit with the highest flux of cosmic radiation and exomaterials. The sun is entering a solar minimum, sun spot activity is dramatically lowering and the earth’s geomagnetic field is changing, directly impacting the planet and allowing cosmic radiation to penetrate the ionosphere. Interesting, COVID19 disease exploded across the world at the exact peak of the March equinox, the exact time correlated to anomalous geophysics during a solar minimum, with smaller peaks globally in the October equinox. Interestingly, in December 2019, a few months before the pandemic, the sun had 33 solar flare free days in a row, setting a record in known history and indicating we are in a “deep” solar minimum. Not only are we in a deep solar minimum, but based on changes of Helium presence in this cycle, it appears there are fundamental mechanistic changes happening in the sun.

This sounds crazy, that the sun could effect disease on earth, but the influence of cosmic radiation and our connection to the earths geomagnetic field is not a new concept. Diseases, particularly viruses, come in yearly cycles and nobody seems to know why, but each virus seems to have its own, very different cycle. A good resource is the science magazine article: Why do dozens of diseases wax and wane with the seasons — and will COVID-19?
Geophysics and Pandemics:
A famous astrobiologist, Professor Chandra Wickramasinghe, predicted a 2020 pandemic based on geophysics conditions and wrote a paper, “Is the 2019 novel coronavirus related to a spike of cosmic rays?”. A detailed paper presented at a NASA conference and hosted by Harvard, lays out conditions for a pandemic triggered by solar radiation. A detailed paper reviewing pandemics since 1700 indicates that the disease outbreaks in 1918, 1957, 1968, 2009 and current correspond to solar minimums. GrandSolarMinimum.com publishes ebooks and information on solar activity and disease and in 2018 predicted an influenza outbreak in this solar cycle minimum. A forward looking pre-print published in November 2019 analysed the mysterious 2019 “vaping illness” outbreak and connected it to a geophysical mechanisms which was (correctly) predicted to be responsible for a future outbreak in 2020. A group of well respected government astrophysicists and doctors has developed a very detailed statistical model around disease cycles driven by “solar pumping”, which also explains cyclical outbreaks of COVID19, and explains why influenzas often have a yearly cycle but its offset based on geographical latitude and not climate.
Geophysics and virology have made crossroads before, with the spread of disease often correlating to distance from the equator and time of year and not just climate. More than 50%+ of astronauts experience reactivation of dormant neurotrophic viruses like human herpesvirus, Epstein-Bar, HSV, CSV and VZV — all known neurotrophic viruses, while on shuttle flights or on the international space station. It is assumed that immune stressors are the cause of these reactivations, but the same immune stressors on earth do not create the levels of reactivation seen. Its possible that cosmic radiation or changes in biophysics of the astronauts bodies are responsible for the reactivation events. Interestingly, reactivation of multiple dormant neurotrophic viruses has been seen in COVID19 in multiple papers and anecdotally many COVID19 patients have tested positive for Epstein-Bar antibodies.
In terms of cosmic radiation, geomagnetics, etc. Across the board these researchers agree that the Equinox’s (March/October) are the time each year where these effects are most relevant and mass casualty events can be expected. One reason is the Russel-McPheron effect, during these times the ionosphere contains cracks, allowing cosmic radiation and “solar wind” to become geo-effective. The direct changes in the geomagnetics of the earth are seen during these times, which could potentially interact with biological systems directly as discussed later.
The concept of “Space Weather” effecting human health is not new, just not mainstream. Large groups of researchers and hobbyists produce forecasts of space weather events and how they may effect life here on earth, which can predict days where cosmic radiation, solar winds and geomagnetic changes may effect health. These groups like SpaceWeatherLive.com and Suspisious0bservers have large followings and contain word class researchers from institutes like NASA.
Anomalies in SARS-CoV-2 Spread and Fatality:
The anomalies in SARS-CoV-2 causing the 2020 mass casualty events through traditional contact spreading are seen by looking at places which should have been ravaged by coronavirus, yet are mostly unaffected: almost all of Asia and Africa — its like this magic virus just skipped some continents. India is an excellent example, in the commercial slums of Mumbai, almost 6 million residents live in high density urban housing with unsanitary conditions and are not able to isolate due to poor economic conditions and communal bathrooms — yet a recent sero survey showed that 60%+ had antibodies after a coronavirus outbreak, with a reported fatality rate which is less than the flu. This makes no sense in the context of Wuhan’s estimated 6%+ fatality rate, which was not seen elsewhere and no genetic analysis or mutation data has been able to correct for this.
The only controlled study of COVID19 infection and public mask wearing shocking found that wearing a masks did not statistically effect the rates of positive SARS-CoV-2 PCR tests. While masks not preventing COVID19 in the wearer seems to contradict scientific consensus and many other studies, its important to remember that these previous studies look at “case number” data from locations before and after restrictions, without adjusting the data, and do not account for locations which may refute their hypothesis — of which there are many. This is important as testing policy continuously changes, such as: whether antibody tests count as a positive case, whether contact tracing counts as a positive case, PCR kits with different false positive/negative, PCR cycle numbers, availability of tests and testing access policy, etc. Any changes in the mentioned variables introduces a sampling bias and to date no research papers linking public mask wearing to infections has accounted for this, expect for the study which found masks to have no significant effect. This should not effect public health policy as wearing masks could potentially protect the wearer from infecting others, but as for preventing the COVID19 disease state for the wearer — it seems to have very little bearing.
It is critical to perform “human challenge” experiments to see if SARS-CoV-2 human to human transmission in a controlled environment correlates to severe COVID19 disease state. The first SARS-CoV-2 “human challenge” experiments were announced October 20th and will infect 30–50 participants with increasing doses of SARS-CoV-2 until disease presents. If the bioenergtic theory of COVID19 is correct, no matter how high the dose of SARS-CoV-2, participants will not get severe disease or “long covid” effects. Studies early in the pandemic showed multiple people quarantining in a household together for long periods of time with sick patients and not spreading the disease. Interestingly, a meta analysis of 54 studies with 77,758 participants found that for a patient ill with COVID19, there is only an 18% chance they will infect someone at home and 0.7% if they are asymptomatic. The largest nucleic acid survey, over 10 million people in China found that asymptomatic transmission had never occurred — this is very strange for the current understanding of a highly infectious and high fatality rate virus that was reported to spread to more than 20 countries almost instantly and caused mass fatality.
Looking at the data it seems there were environmental effects driving fatality in this pandemic with graphs of deaths highly coupled across vastly different geographic zones. Anecdotally, speaking with people around the world, most indicate they fell ill during the mid March equinox, or even mid 2019 and were told there is no way it could be COVID19, many of them still suffering with “long covid”.

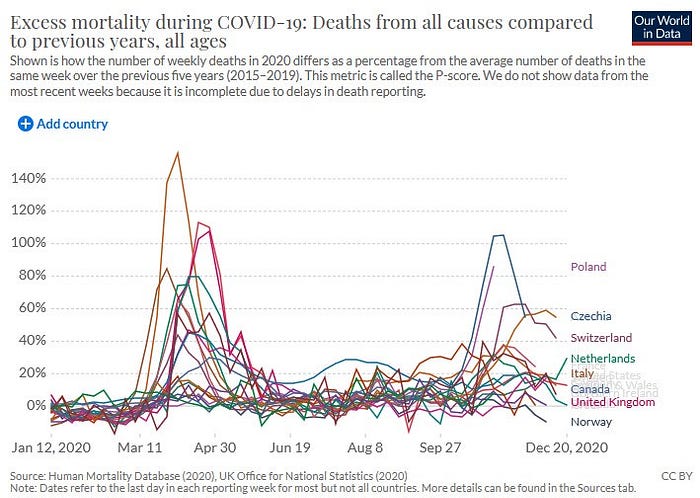
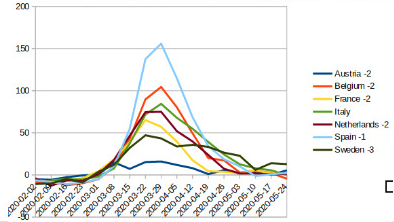
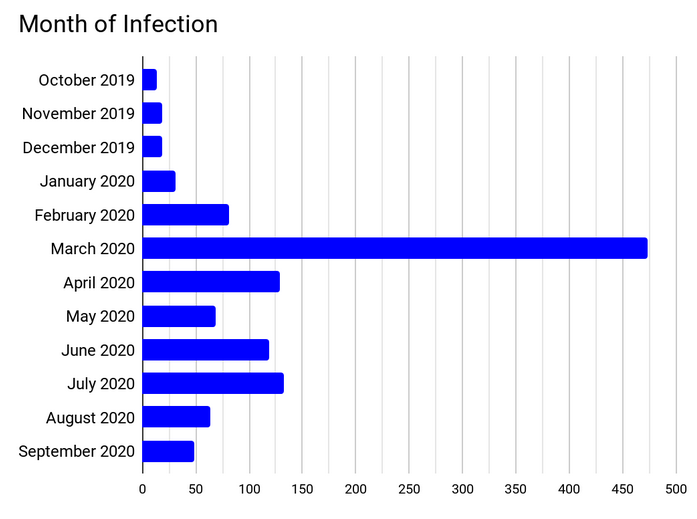
Its obvious that there are mass casualty events due to a new COVID19 disease in 2020, but what if in very particular areas with geomagnetic anomalies there are spikes in death? These are questions that need to be asked during such a mysterious pandemic. Excess deaths spiked across the world in areas with dramatically different climates, populations, travel from China — all at the same time, as can be seen in the following graphs:
Sweden is an interesting control for watching the spread of COVID19, as they chose light and voluntary social distancing measures, with nightclubs and restaurants open and the general public not using masks. Sweden’s chief epidemiologist is puzzled by what they are seeing, in a recent interview he stated: “What we are seeing now in Sweden is a rapid decline in the number of cases, and of course some sort of immunity must be responsible for that since nothing else has changed.” Tegnell credits “some sort of immunity” to the lack of deaths in Sweden, but in October, after months of light restrictions and flat death rates there was a spike of fatality — indicating the lack of deaths had more to do with external factors than population immunity. Tegnell states, “This disease appears to work in a different way. The spread is more patchy, so the likelihood is greater that we will see — as one is currently seeing around Europe — outbreaks in certain places, at workplaces and similar environment”. In previous interviews, Tegnell states, “It’s a little bit of a mystery why nothing has really happened in other parts of Sweden. The virus keeps on surprising us when it comes to this” and “every country’s different, the epidemic looks different in every country and I don’t really understand completely why.” Its clear there is some environmental factor not considered.
Kinsa Healthweather is a health dashboard operated by a smart thermometer company with over one million smart thermometers around the US reporting data. In early March the CEO made a statement, “While we cannot definitively say this is showing COVID-19, we CAN say that we are seeing unusually rapid spread in illness. Today, that is presumably COVID-19. It is imperative we start to use this system, and similar tools, to stop the spread of COVID-19 and ultimately prevent the next outbreak”.
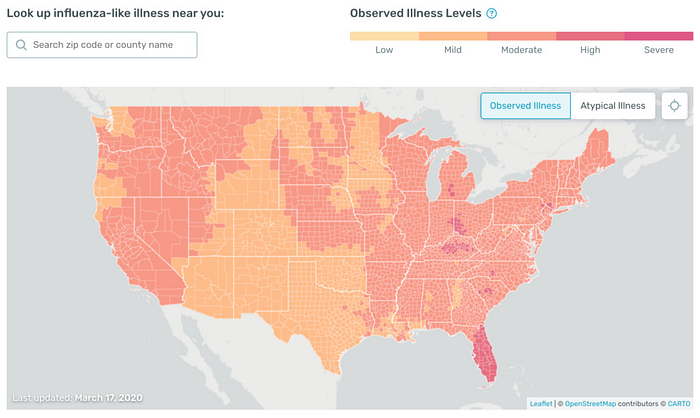
Historical data from the Kinsa Healthweather dashboard has been removed (it showed nothing since compared to the March event) but one data scientist scraped the data into a database - fever data for over 100,000 US counties. Tabulating the fever data based on date across the entire United States, shows a peak which lines up with the peak of fatalities in mid-late March globally.
PCR Testing Anomolies:
The PCR tests used to indicate someone has COVID19 are generating more questions than answers. There is no single country where the number of “cases” corresponds to the number of COVID19 deaths, even when adjusted for incubation period, etc. The two graphs are totally decoupled indicating a failed testing system that does not represent the reality.
Interestingly, the standard for the PCR tests is to amplify the viral material in “cycles”, with more cycles amplifying more material, with the caveat that too many cycles can create false positives or amplify RNA irrelevant materials. As Karry Mullis, the Nobel prize winning inventor of PCR states: PCR should never be used as a medical diagnostic. The standard for the COVID19 PCR tests is to operate them at 40+ cycles, meanwhile Dr. Anthony Fauci himself states that 35 cycles is an unofficial standard as anything above that will test positive on “junk nucelotides” that is not “replication competent” viral material. Interestingly, the World Health Organization released a statement indicating that PCR has a high amount of false positives due to inherent problems with PCR and the cycle threshold should be adjusted dynamically. In early January 2021, the FDA released a statement warning of the misleading results of PCR testing, joining the WHO in recognizing the poor performance of PCR tests.
Anecdotally, many people with textbook COVID19 symptoms do not test positive, while many people with no symptoms test positive and are called “asymptomatic”. In fact, one person taking multiple tests in a single day can receive multiple test results, a nightmare for public health. The PCR tests have never been gold standardized and were developed rapidly in the earliest days of the pandemic, highly leveraging theory guided sequencing. In that context, what is COVID19 disease state and why does it not correlate to SARS-CoV-2 viral load?
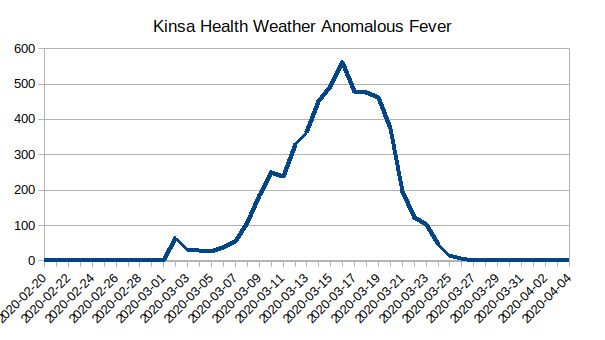
One of the only studies to show viral load via daily PCR tests and serial cycle threshold values of hospitalized patients, found that the viral load oscillated dramatically over the course of even severe COVID19 and did not seem to correlate to disease progression.
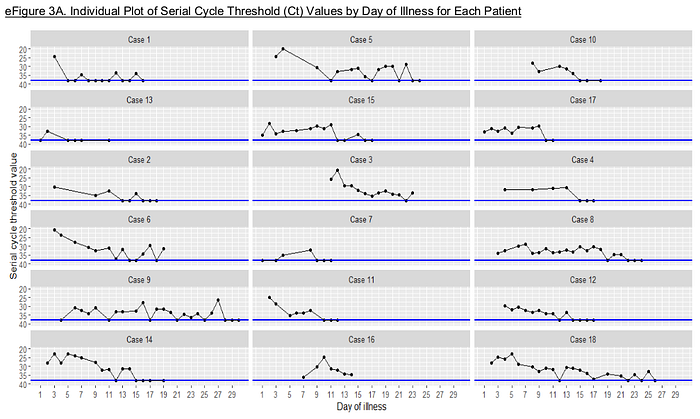
A freedom of information request was used to collect PCR cycle data from over 5000 COVID19 tests at a state lab, this excellent analysis shows average PCR cycles required for a positive result over time — Low cycle values after the March equinox, dramatically increasing to PCR cycles that indicate a “non-replication competent” viral material load as time goes on. This increase in PCR cycles required also correlated with a dramatically decreased fatality per day in the local area.
Many might look at the data of increasing PCR Ct values as time goes on and claim it is due to social distancing and a dropping viral load, but the relationship is linear, representing a decay over time and not an abrupt cutoff as contact conditions rapidly changed overnight with social restrictions. This trend in PCR cycle values should be investigated.
Potential Mechanisms:
The biochemistry of COVID19 provides indications that it is a bio-energetic disease — highly involved in cell oxidation, cell energy systems and involves electromagnetically susceptible iron. As I wrote about previously, the only group of doctors with a theory of COVID19 long term morbidity that is successfully treating patients and giving “long haulers” their lives back, believes the NAD+ energy system of the body to essentially be drained in COVID19. This leads to important cofactors being scavenged and depleted, chronic NAD+ depletion and long term dysfunction of metabolically active organs — causing all of the complex and evolving issues across seemingly all systems of the body. Interestingly, this NAD+ system dysfunction, is highly linked to the PARP (poly ADP ribose polymerase) system, a critical system activated in the body when oxidative damage causes single cell DNA breaks.
Their research, COVID-19: NAD+ deficiency may predispose the aged, obese and type2 diabetics to mortality through its effect on SIRT1 activity, has received an excellent response and seems to be validated in mice, relevant abnormalities found in ferrets and the mechanism echoed by other researchers. Dysfunction of relevant systems are found in COVID19 and correlated with inflammatory markers. Clinical trials are under way to treat the same mechanism using more exotic and commercial compounds than the simple ones used with success in their case.
According to this theory, cofactors coupled to the oxidation/NAD+ cascade are critical to outcomes and this is seen in the observation that low selenium levels correlated to poor outcomes in China. Observations of high blood sugar being a predictor of death in COVID19 patients, regardless of diabetic status validate metabolic changes being a major risk factor of COVID19 according to NAD+ theory. Activation of the same kynurenine pathways predicted in NAD+ theory of COVID19 correlate to blood sugar deregulation.
All of the complex and strange morbidity of COVID19 could be explained by spontaneous oxidative stress causing single strand DNA breaks. Recently, a paper was published which reviewed biomarkers of oxidative DNA damage and found a strong correlation to COVID19 severity. Another paper which looked at Ascorbate levels which would be reduced during oxidative stress, states: “Our study revealed that vitamin C levels are undetectable in more than 90% of the patients included. The mechanisms of this significant reduction in vitamin C are uncertain.” A study of antioxidants as well as biomarkers of oxidative stress in COVID19 patients shows dramatic patterns of low antioxidants and high oxidative stress. Thiol levels, a common biological group very sensitive to oxidation is highly correlated to COVID19 disease progression in a recent paper. The serum thiol biomarker levels tested are considered a direct measure of redox status because of their rapid reaction with oxygen radicals.
Its often mentioned that COVID19 causes “cytokine storm”, but this is not a normal cytokine storm, a recent paper analysed the immune cascades and pointed out the “cytokine storm” in COVID19 is less severe than influenza. It looks a lot more like systematic inflammation of another cause.
“Long Covid” is a debilitating new disease state many suffer from after COVID19 infection and an important window into understanding COVID19 mechanisms. The NAD+ theory of COVID19 indicates these long term effects are expected due to almost a type of intracellular pellegra, a fatal disease of vitamin B3 deficiency as well as disruption of metabolically active tissues like the brain and other organs, and the results of circulatory serotonin depletion leading to mast cell activation. Most “Long Haulers” taking nicotinic acid (form of vitamin B3) as well as NAD+ synthesis cofactors seem to recovery rapidly. Interestingly, “long haulers” also provide a window into understanding the temporal dynamics of bioenergetic disruption, a survey from a patient advocate group of 1,200 long haulers indicates that the majority of those with “long covid”, got sick during the March peak. Anecdotally, many “long haulers” who become sick early on felt that they had a “reactivation” or “reinfection” during the October peak.
IncellDX, a company operated by a stanford Virologist, Dr. Bruce Patterson has developed a diagnostic test kit that can determine with 98%+ accuracy who is suffering from “long covid”. The IncellDX algorithm uses the following cytokine/chemokine biomarkers: IL-2, IL-4, IL-6, IL-8, IL-10, IL-13, CCL3, CCL4, CCL5, TNF-a, sCD40L, IFNY, VEGF — indicating those with “long covid” are suffering from systematic inflammation over the long term.
An interesting study observed compounds (Isoprostanes) in community sewage to estimate oxidative stress and found an increase in March and then a return to baseline the next months, which lines up with fatality rates, anomalous fevers, PCR Ct thresholds and the maximum geo-effectivness of solar radiation and magnetic anomalies.
Looking at the correlations to fatality, there seem to be two baskets: iron metabolism and oxidative repair cofactor depletion. In the context of spontaneous oxidation throughout the body and disruption of the bio-energetic NAD+ system. Iron could be a smoking gun — Iron causes oxidation in the body through energetic oxygen radical production, including via the extremely powerful Fenton reaction. The production of these radicals and oxidative molecules are the missing key which could cause the single strand DNA breaks leading to the COVID19 disease state. Most interestingly, A recent paper cleared up the misconception that the the fenton reaction from excited iron in cellular systems damages DNA with the strong hydroxy radical mechanisms, it actually damages DNA with the low energy carbonate anion radicals. Carbonate anion radicals are specific for complex guinine containing sequences. This explains the observation of guinine oxidation products correlating with COVID19 disease severity.
There is strong indications of disruption of iron homo stasis in COVID19 — the paper “Iron: Innocent bystander or vicious culprit in COVID-19 pathogenesis?” reviews mechanisms and findings connected to iron in COVID19. Multiple papers have found that large amounts of free iron in the body are correlated to fatality, blood types with higher iron binding capacities correlate to fatality and iron dynamics are significantly interrupted in COVID19 patients. Iron is also a critical mechanism to mediate bacterial infections and forward looking research shows anomalous presence of bacterial DNA reads and biomarkers in COVID19 clinical data indicating attack of iron utilizing anaerobic Prevotella sp. bacteria on the blood.
COVID19 may most similarly mimic cadmium poisoning, where a catalytically active metal is causing systematic oxidative stress. It is relevant to note that in cadmium poisoning, there symptoms overlap perfectly with COVID19, including “cytokine storm”, anosmia and ground glass lung opacities. The cadmium poisoning mechanisms have been well studied and an analysis will show its close relationship. Combined with the many papers linking COVID19 and systematic oxidative stress, it paints a picture which looks more like an oxidative disease than a traditional viral infection.
In the context of PCR testing and bioenergetic triggered disease its important to note that the PCR tests detect short RNA fragments, often less than 25 nucleotides and could potentially be triggered by rogue DNA/RNA fragments not only from our own cells but also microbiome after destruction. A recent publication reviewed free DNA in the body and its correlation to disease state and found some astounding correlations. The level of free DNA corresponded directly to disease outcomes and clinical severity and was significantly higher in COVID19 than any other previous virus.
This paper had multiple shocking findings; Not only did COVID19 highly involve DNA fragments in circulation, but patients treated with experimental antivirals, experimental immunsupressives, hydroxychloroquine and/or the standard of care did not have changes in free DNA, as if the viral load was not correlated to free DNA. Its relevant to point out that free DNA itself can trigger cytokine storm and tissue damage.
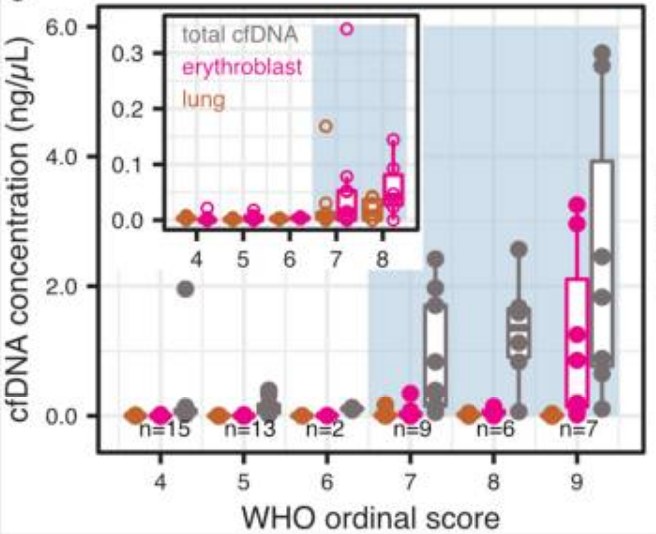
Even more shocking was that a large percentage of this free DNA came from erythroblasts, the red blood cell precursors found in the bone marrow. This is a shocking discovery as damage this aggressive to the red blood cell precursors in the bone marrow can not be easily accounted for by any current viral mechanism. Interestingly, erythroblasts contain a large amount of iron and a structure that is not stable and resistant to auto-oxidation like mature red blood cells. As erythroblasts contain iron and undergo rapid mitosis, they are one of the most radiosensitive tissues in the body.
The final key to understand a potentially new type of disease is: what is exciting the iron to create single strand DNA breaks, oxidative stress and blood dysfunction?
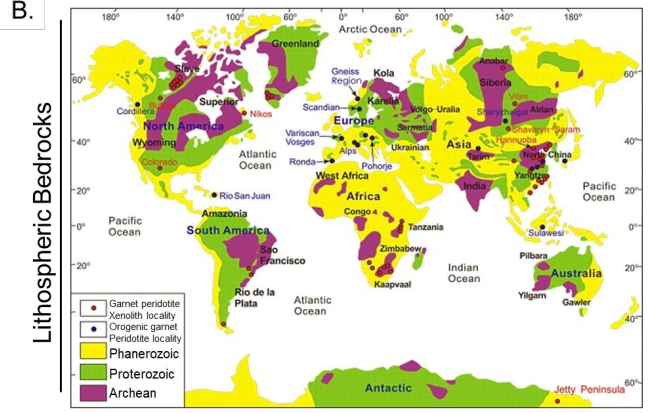
One researcher speculates that geomagnetic coupling to the iron in the body causes catalysis and triggers oxidative stress through iron mediated oxygen radical production. He speculates that during these solar minimums and most particularly around the Equinoxes in March and October, the Long Wave Magnetic Anomalies excited iron containing Proterozoic bedrocks, which then relax and couple energy in the iron molecules of the human body — leading to oxygen radical production, DNA breaks, oxidative stress and in those succepptable in high flux locations — the COVID19 disease state. While the final step, the long wave magnetic coupling between Proterozoic rocks and human blood involves physics mechanisms that are forward looking — it makes sense in the context of energy/matter integration.
This interaction of long wave magnetic anomalies and cellular iron/radical production processes is currently beyond the grasp of science, but a recent paper disrupted our understanding of organisms interaction with geomagnetism when it showed that weak magnetism fundamentally changed a cell cultures fluorescence.
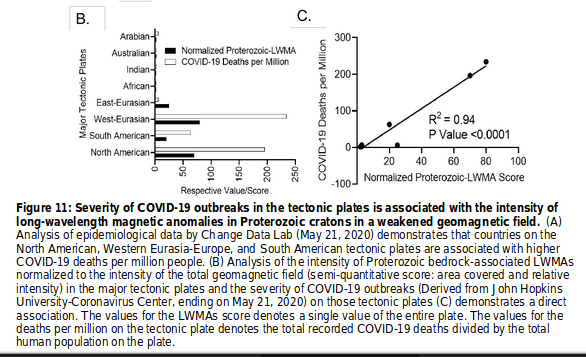
This is interesting as it explains the strange spread of COVID19 disease — by correlating Proterozoic bedrock which could couple geomagnetically and known low strength of the geomagnetic field, a scoring system can be created for risk of bioenergetic disease.
Its speculated that this mechanism was the cause of the “Vaping Illness” which had the same lung damge, symptoms, fatality rate and disease demographics as COVID19, due to Long Wave Magnetic Anomoly events in mid 2019 — amplified by smokers using iron containing vaping devices or potentially due to oxidative stress catalysis from the pyrolysis of Vitamin E acetate. Duroquinone is a Vitamin E pyrolysis product and can trigger catalysis of oxidative damage cascades in the lung. Its important to note that this work created the only time correlated prediction of mass casualty events in 2020 — the ultimate validation of scientific theory.
The correlation of conditions which would align to create bioenergetic disease is highly statistically significant, both in terms of location and time. The follow graphs show first the location and then the timing of COVID19 deaths:
If these ideas are correct there will be another mass casualty event around the world in places which previously had “outbreaks” in March 2021 with an unknown magnitude. This peak provides an important window to observe and learn about bioenergetic disease states.
“Long Covid” overlaps with Chronic Fatigue/Myalgic Encephalomyelitis:
COVID19 has many parallels to Chronic Fatigue Syndrome and Myalgic Encephalomyelitis, two diseases which are becoming more and more common. ME was coined after the 1955 Royal Free Hospital Outbreak, where 292 members of the hospital staff fell ill with a mystery outbreak. The symptoms of the Royal Free Outbreak are virtually identical to some of the strange findings in COVID19, including non-specific EEG abnormalities, something that would be expected in the case of a bio-energetic disease. It would be important to point out that the Royal Free Hospital Outbreak happened during a solar minimum in 1955, in a location where COVID19 is having high fatality rates and is susceptible to geomagnetic anomalies.
Another very important event is the “Tahoe Mystery Illness”, a similar situation which happened in the town of Truckee, also during a solar minimum in 1985 that later spun out the recognized “Chronic Fatigue Syndrome”. According to a statement on a news report, Rumors out of Truckee, “People were catching this strange flu, and they just weren’t recovering. If someone caught this flu and got over it within about 3 weeks or so, it seemed like they were pretty much out of the woods, if it went on any longer, 4 weeks or longer, the rumours said they wouldn’t get any better, and in some cases got worse”.
I have interviewed Erik Johnson, a key patient in the original CFS cohort and resident of Truckee at the time
Erik Johnson Interview
Nikita Alexandrov:
You were at “ground zero” of the “Tahoe Mystery Illness” which was later renamed “Chronic Fatigue Syndrome” in 1985. Its very interesting as there are so many parallels to the 2020 bioenergetic disease events — it happened during a solar minimum, everyone across the board in Tahoe seemed to get sick and it led to chronic disease, just like we are seeing with COVID19 in 2020. Could you tell us about the background of Tahoe Mystery Illness/CFS and your involvement?
Erik Johnson:
I’m a survivor of the 1985 “Lake Tahoe Mystery Illness”, renamed in 1988 by the Center for Disease Control, “Chronic Fatigue Syndrome”. My background is Army Nuclear Missile Launch Specialist, deployed in Germany 1975–1978, I received Biowarfare Training in the Army and am trained to look for the signs of biowarfare attacks, what happened at Lake Tahoe was much different.
I spend my time as a patient advocate for CFS, teaching people about the early history as I was “In the Room” when CFS was being classified and saw the whole process. I was the first patient selected to be a “prototype” for the Holmes 1988 CFS definition. So I am particularly interested in comparing the 1985 “Tahoe Flu” to Longhauler syndrome.
I was also diagnosed by the three ME literate specialists who were in the 1987 Holmes committee as having “all the primary determinants of ME” — Drs Byron Hyde, Gordon Parish and Alexis Shelokov.
They were analysing the Lake Tahoe outbreak patients and these ME specialists were so angry that the CDC was going to create a new syndrome that they walked out in protest.
There is a very specific reason why I was chosen as the first prototype for this new syndrome, the CDC was fooled by the reactivated EBV but I was one that did not have it. Dr Paul Cheney found that the fluctuating titers to EBV were a surrogate “immune function test”, not of EBV itself, rather, a red flag for an immune system that was failing to keep the common EBV in restraint. Dr Cheney looked for EBV negative patients to use as examples to show that EBV was neither inherent or necessary to the syndrome. He tested us all, to find the minority who don’t have EBV, eventually finding 19.
I was the first, we were known as “the pristine cases” and served as the basis of the CFS syndrome. As you can see, doctors did not agree, they adopted the CDC view that you either have EBV, or you don’t. They knew what Dr Cheney was doing, but refused to accept his premise, because this scared them so badly, the implication was that something unknown was destroying immune function at Lake Tahoe.
He believed that an “activator virus” was weakening the immune system, allowing EBV reactivation, but he, and all researchers, looked very hard to find one, and could not. This seemed to scare people, the idea something unknown was making people sick, many scientists and officials just stopped asking questions and started ignoring evidence at this point.
Nikita Alexandrov:
Can you speak about your observations on the ground, mass illness etc? You mentioned that animals got sick, during March 2020 in Vancouver, I witnessed the Canadian geese flying migration patterns in circles, being aggressive, flying around in the middle of the night non-stop for the first time and it seemed like everyone in the city was just a bit ill— what did you observe?
Erik Johnson:
There was a base value illness that hit all at the same time, it seemed little more than food poisoning or a mild flu, but it hit everyone at the exact same time. Even the pets got sick, as well as animals. The chickadees lost their song, the geese stopped migrating, they stayed at Lake Tahoe in large numbers. Their solution was to shoot them, they hired professional shooters to wipe them out, I couldn’t believe it.
The earliest signs of “Sick Building Syndrome” were starting to appear.
This was noted by doctors, but they did something bizarre, they shut off their minds to it. There were massive mold outbreaks in the buildings. A huge algae bloom, but this was blamed on the geese. There was a giant crayfish die off, millions of them. Even all the frogs died, I have never seen anything like it.
It was almost like the air lost its vitality, even the trees looked sick. I have never seen any of this stuff before or since.People were so scared that they thought an ancient volcano was stirring, emitting toxic fumes. When our incident happened, everyone was full of static energy. Even pets, dogs would sniff a car door and whimper as it shocked their nose. Cats and dogs would walk on carpet and lift their feet at the power of static shocks.
The lightning changed, growing up at Tahoe the lightning was always huge vertical pillars, the lightning became thin and multi forked. Always moving laterally and never vertical, crazy bad lightning. This struck me as being from charged particles similar to what is seen after a nuclear explosion. That lightning was also unparalleled by anything that happened since.
This was all very strange and no one had ever seen it before. Lots of crazy things happened. Each doctor seized on the first virus or bacteria he identified, blamed that, and ignored everything else. The rate of sickness is now massive, Dr William Rea called Truckee “Cancer capital of the West” When the new syndrome was coined, everyone went in different directions with their own theories, the CDC encouraged this.
-end interview
These bioenergetic events seem much more common than we would expect, leading to chronic disease, most likely through the unbalancing of the NAD+ system. The book, “The Clinical and Scientific Basis of Myalgic Encephalomyelitis — Chronic Fatigue Syndrome” has published a large list of “outbreaks” leading to chronic fatigue syndrome.
Biomarkers of DNA breaks and oxidative stress should be monitored over time during the next equinox, particularly in areas which previously had high levels of fatality with COVID19. Monitoring of long wave magnetic anomolies would be a good correlation and their may be increase dissolved hydrogen in the ground water in areas with spontaneous serpentization leading to long wave magnetic anomalies — if this theory of bioenergetic events is correct.
Bio-markers to screen to detect bioenergetic disease states:
Ascorbic acid levels — biomarker for general oxidative stress*
y-H2Ax histones — biomarker for double strand DNA breaks
8-oxodG — biomarker for DNA oxidative stress**
cfDNA — circulating free DNA
Edit — A paper was published which found (as expected according to the base mechanisms of this theory) nearly non-existent Ascorbate in COVID19 patients, “Our study revealed that vitamin C levels are undetectable in more than 90% of the patients included. The mechanisms of this significant reduction in vitamin C are uncertain.”.
Edit — Since publication of this post, a paper was published which found a strong correlation between 8-oxo* biomakers and COVID19 severity, further validating the base mechanisms of this theory.
COVID19 as a bioenergetic disease is great news, it means there are bioenergetic solutions. The mass casulty events will be highly predictable, peaking in March and October of every year and reliant on that years solar cycle. Space weather may be just another weather station, with geomagnetic anomaly warnings being similar to tornado warnings. Taking compounds which scavenge oxidants and support DNA repair will dramatically decrease fatality, moreso than any antivirals. Devices could be potentially used to neutralize geomagnetic coupling to human bodies, with a single antenna system serving large community areas.
According to the bioenergetic theory of COVID19, global mass casualty events will be triggered in March 2021, depending on the intensity of specific aspects of the 2021 solar cycle, which can be determined months before the events. Events will take place in locations which previously had high percentages of fatality and can be predicted by overlaying geomagnetic field data with Preterozoic bedrock maps. The increase in spontaneous deaths in March 2021 will follow the exact same trend as 2019, hitting Italy initially and will most likely be blamed on a new “Italian strain”. The deaths will move upward through western Europe before starting in the US and UK in the same pattern as 2019.
Natural products which support anti-oxidant, genostability and DNA repair mechanisms may be an important prophalaxis including: Vitamin C, Vitamin D, Niacin, Zinc, Selenium, NAC, ALA and Quercetin.
- Talk to your doctor before any changes in diet, supplementation or exercise.
For a more detailed analysis of the suspected mechanisms of “long covid” and potential treatment/prophylaxis, please read my blog post: The Team of Front-line Doctors and Biohackers Who Seem to Have Solved “Long Covid”
“The day science begins to study non-physical phenomena, it will make more progress in one decade than in all the previous centuries of its existence.”
-Nikola Tesla
Nikita K. Alexandrov, BChem, MBA — 12/14/20
“We are waves of the same sea”
Please contact for collaboration/more insight:
NKA369/at/protonmail.ch
